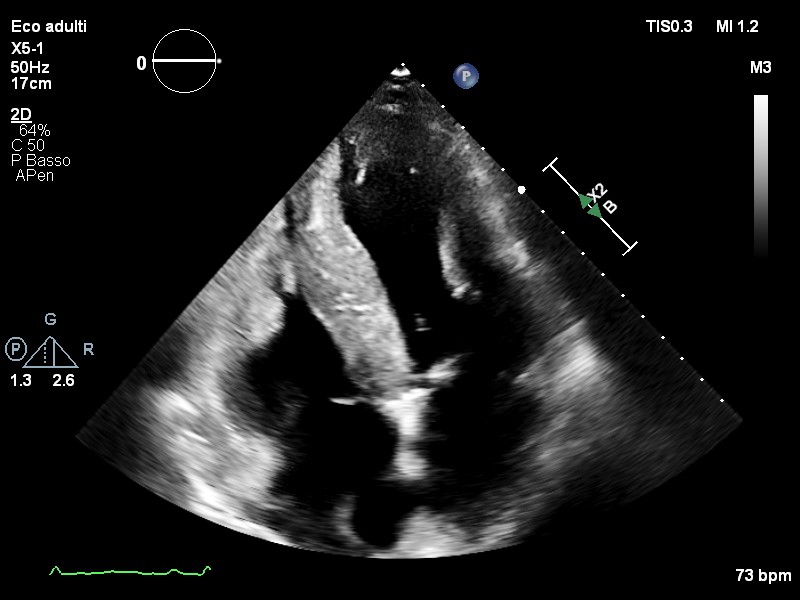
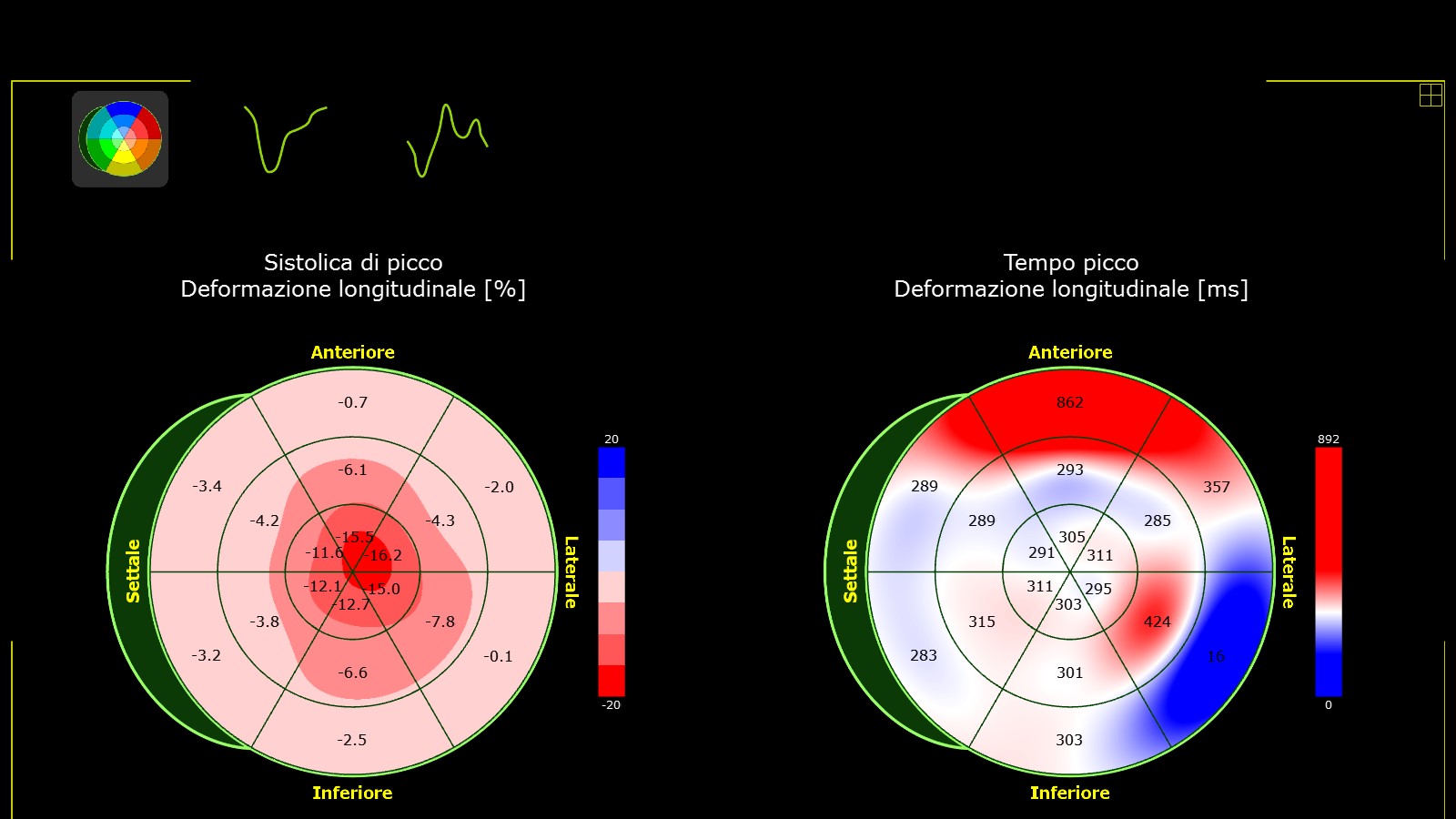
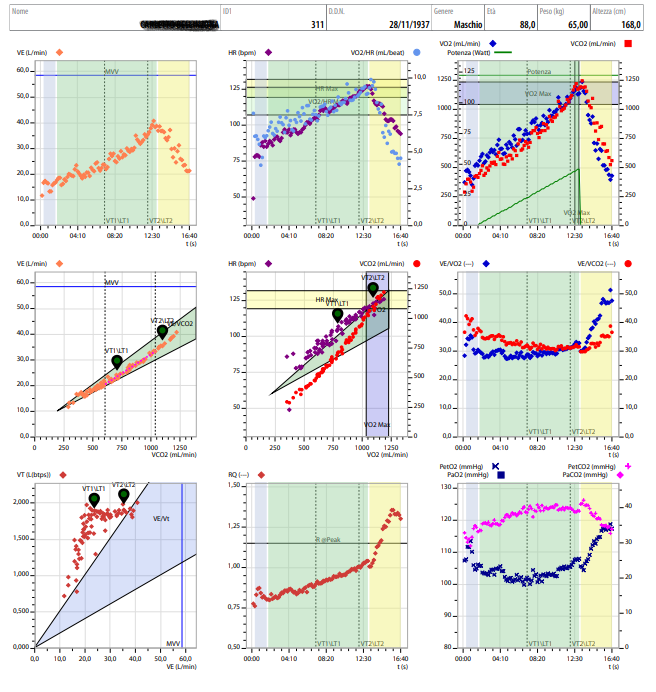
An 88-year-old man with hypertension, dyslipidemia, mild glucose intolerance, and chronic kidney disease (eGFR ~40 ml/min) was reassessed for known wild-type transthyretin cardiac amyloidosis (ATTRwt) , diagnosed in 2022 after an initial episode of heart failure. The patient remained clinically stable and currently reports no exertional dyspnea, consistent with NYHA Class I. Physical examination was unremarkable, without signs of congestion. ECG showed sinus rhythm with low limb-lead voltages. Echocardiography confirmed a non-dilated left ventricle with severe concentric hypertrophy, preserved ejection fraction (57%), and reduced longitudinal strain with an apical sparing pattern. Right ventricular function was normal and no pulmonary hypertension was evident. Laboratory findings showed stable renal function and mildly elevated natriuretic peptides. To obtain an objective measurement of physiological reserve and for prognostic stratification, the patient underwent cardiopulmonary exercise testing (CPET) using a 5 W/min ramp protocol. He achieved a peak oxygen consumption of 17.8 ml/kg/min (94% predicted) with an appropriate chronotropic response, normal rise in oxygen pulse, preserved ventilatory reserve, and a VE/VCO₂ slope of 29.7. CPET revealed a remarkably preserved exercise capacity , unexpected for his age and infiltrative cardiomyopathy. This observation supports the concept that chronological age alone is insufficient to estimate prognosis, functional capacity, or therapeutic suitability in older adults with cardiac amyloidosis. In this context, at AUSL Piacenza a multidimensional geriatric assessment has been incorporated into the pre-treatment evaluation pathway for cardiac amyloidosis, recognizing that frailty, cognition, functional status, and biological age provide a more realistic framework for decision-making. In particular, the use of the Multidimensional Prognostic Index (MPI) allows a validated, quantitative assessment of the patient’s risk of developing adverse clinical outcomes. Within this pathway, CPET adds a crucial functional informations, helping refine risk assessment and therapeutic eligibility. Take-home message: Even in octogenarians, exercise capacity and global physiological reserve may be far better than expected. A multidimensional clinical and geriatric evaluation — complemented by CPET — helps avoid age-based therapeutic exclusion and supports individualized, evidence-based care in cardiac amyloidosis.