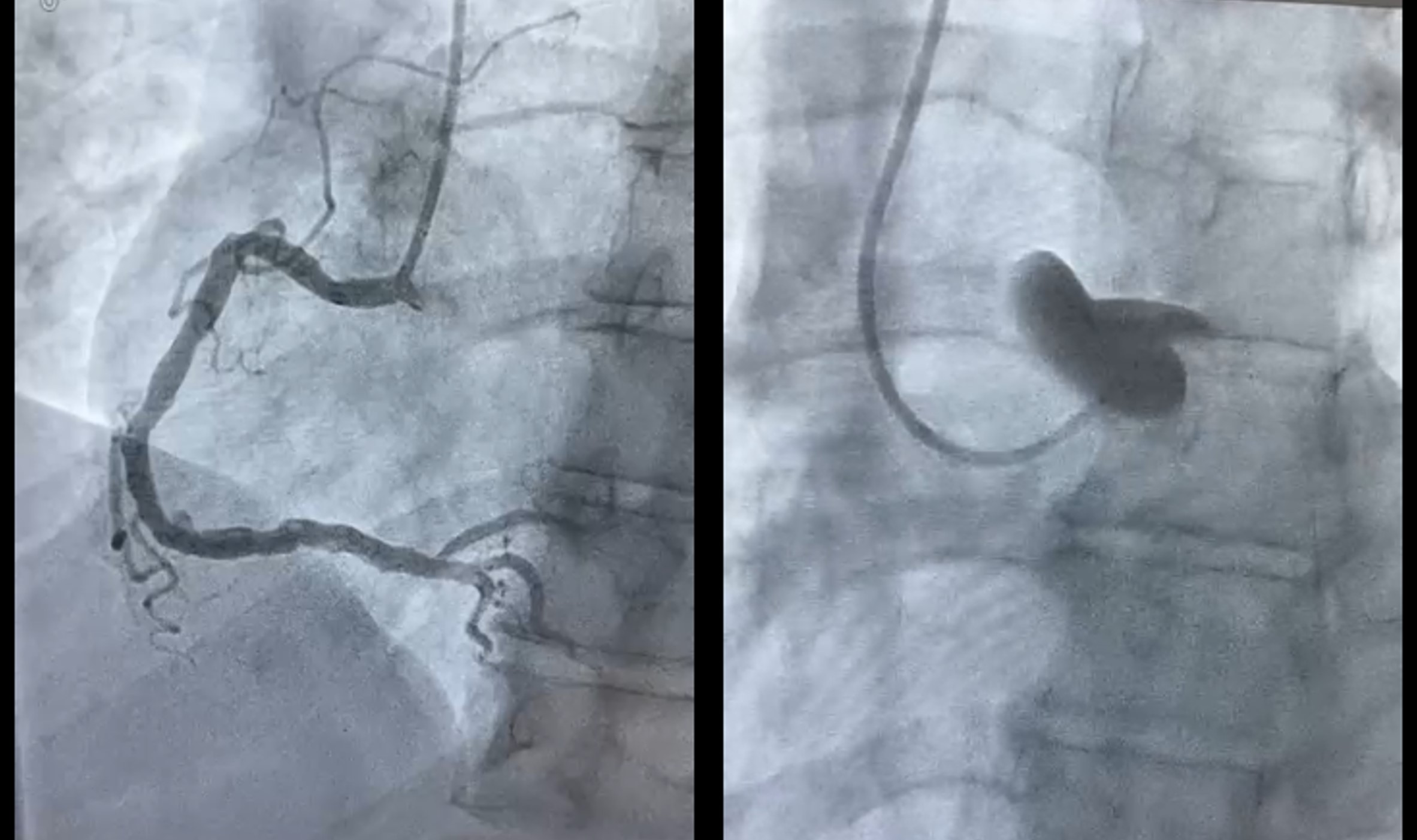
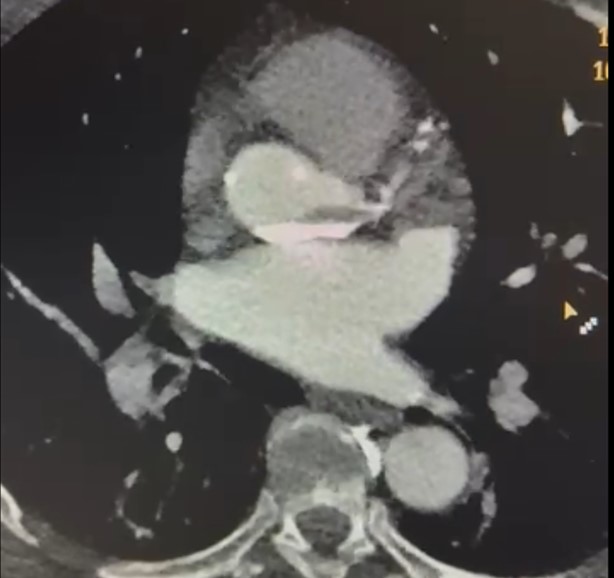
A 52-year-old male patient, with no relevant cardiovascular risk factors or cardiac history, collapsed during a padel match. He was rescued by lay bystanders with CPR and a shockable rhythm, achieving ROSC after one shock. On hospital arrival, ECG showed diffuse ST-segment elevation; the patient remained alert and conscious, with BP 100/60 mmHg, HR 80 bpm, and an unchanged ECG. An IABP was placed, and coronary angiography was performed ( Figure 1 ). The right coronary artery presented non-occlusive disease. During cannulation of the left coronary artery, contrast extravasation was observed, with the diagnosis of acute intramural hematoma. The non-contrast phase confirmed the presence of an iatrogenic intramural hematoma, and the on-call cardiac surgery team was contacted to evaluate the case. The patient's condition rapidly worsened with sudden cardiac arrest. He was therefore rushed to the operating room under CPR. "Blind" myocardial revascularization was performed on the left coronary system using two venous grafts to the LAD and OM, under cardiopulmonary bypass (CPB). The intramural hematoma, assessed as limited and without interference with aortic valve function or antegrade/retrograde progression (TEE assessment), was left in situ. Due to ischemic damage, the patient had severe myocardial stunning and was weaned off CPB with femoro-femoral veno-arterial ECMO + IABP + inotropic support. Considering the lack of early contractile recovery, in the next hours a vent cannula was placed in the left ventricular apex to optimize ventricular unloading. With increased mechanical support and reduced inotropic support, preserved neurological status, and normal right ventricular function, the patient was progressively weaned from VA-ECMO in favor of univentricular support. The femoral cannulas were removed, and the biventricular support setup was converted to paracorporeal left ventricular assistance via the placement of an outflow cannula in the right axillary artery (utilizing the left ventricular apical vent as the drainage cannula) ( Figure 3 ). With this setting, the patient was awakened and subsequently extubated. In the following days, despite observing no recovery of LV function, it was possible to refer the patient to the transplant center, where he subsequently underwent heart transplantation. In conclusion, the patient's priority is established by revascularization, regardless of the presence of other lesions that may modify the surgical strategy