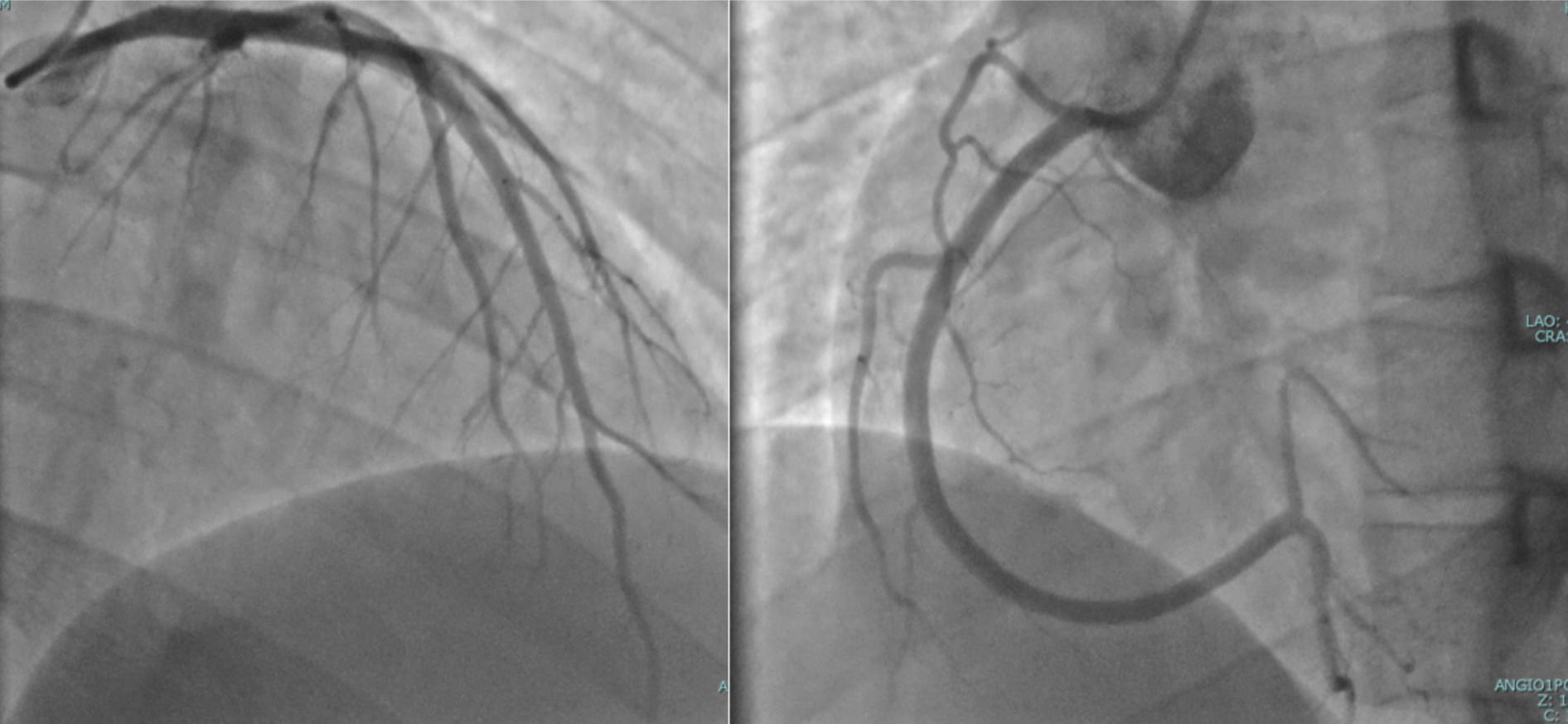
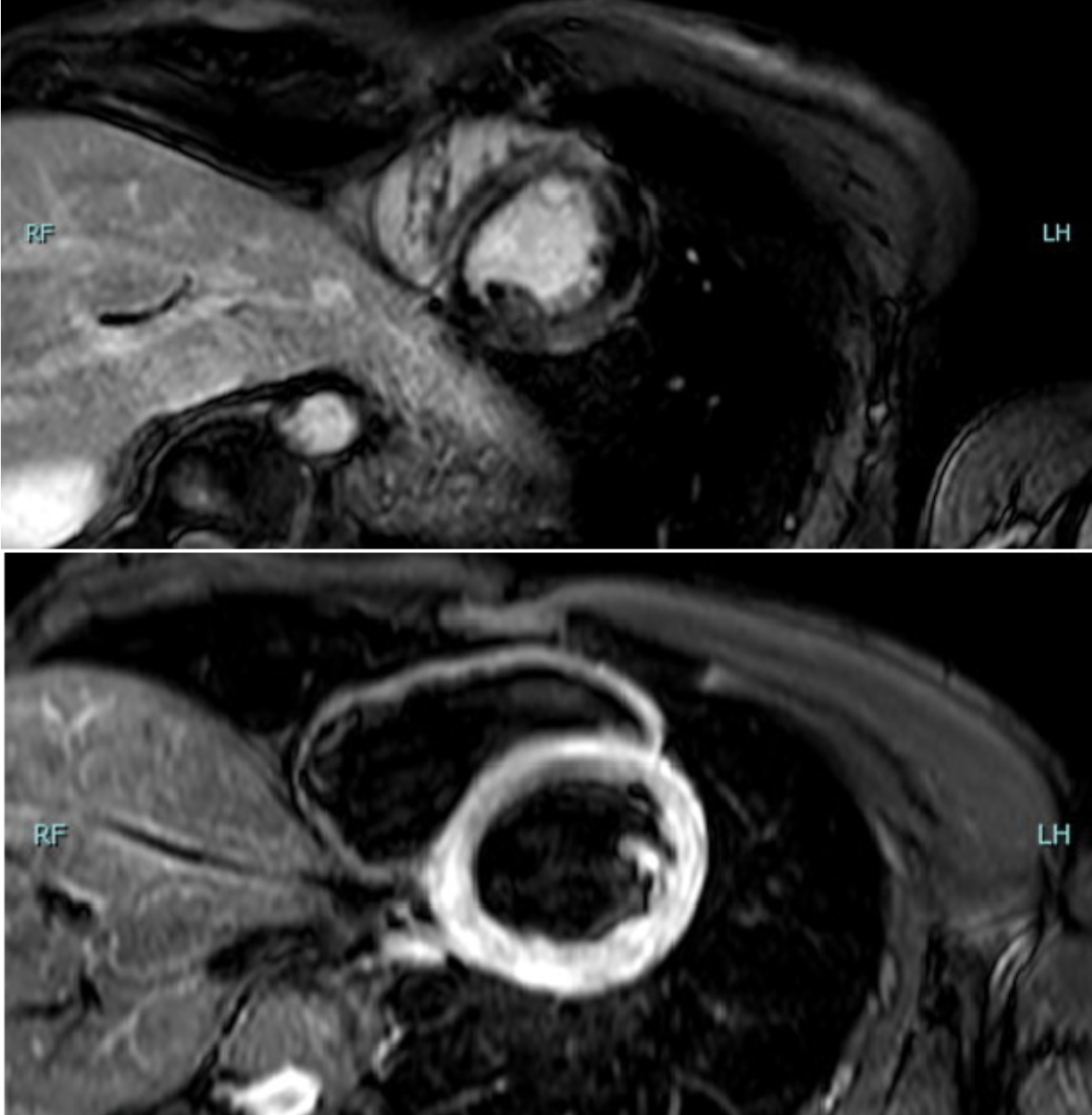
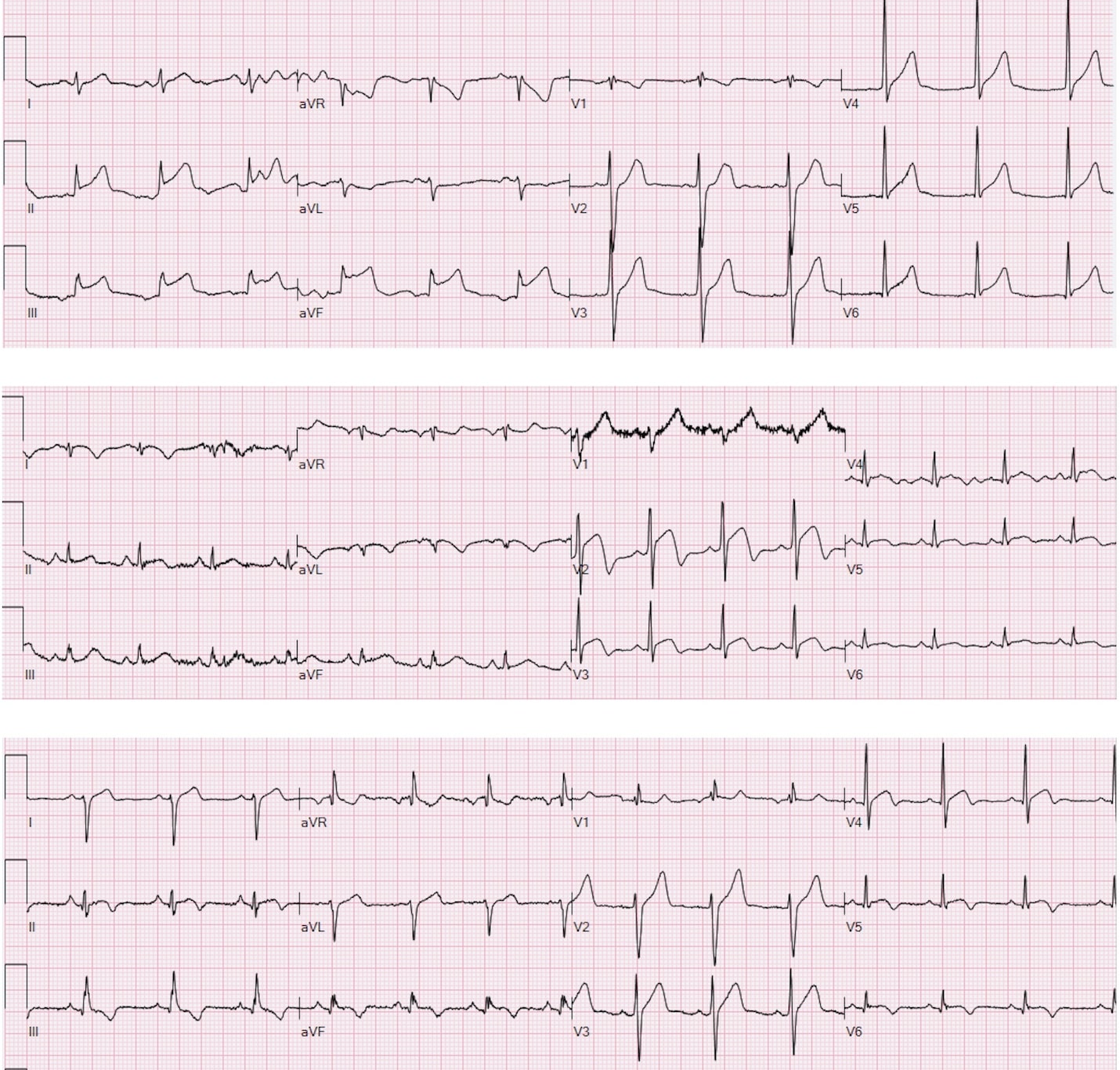
Background. The association between hyperthyroidism and acute myocarditis has been already reported in literature; however, this case presents an unusual scenario without classical hyperthyroidism symptoms or infective myocarditis features, in which the coexistence with thyrotoxicosis suggests a possible but unproven relationship. Case presentation. A 26-year-old male presented with acute chest pain: he denied fever, recent infections or prodromal viral symptoms. ECG performed by emergency medical services showed inferior ST-segment elevation with reciprocal anterior ST depression. Therefore cath-lab was activated; urgent coronary angiography revealed no significant coronary stenosis. Early echocardiography showed preserved systolic function without wall motion abnormalities. Laboratory tests revealed markedly abnormal cardiac biomarkers (hs-TnT peak 3,138 ng/L and elevated CK-MB and CPK) with normal inflammatory markers. Thyroid tests showed nearly suppressed TSH and markedly elevated thyroid hormones (TSH 0.002 mUI/L; fT3 67 pmol/L). Endocrinology consultation prompted further assessment: neck ultrasound demonstrated a normally structured thyroid gland and thyroid autoantibodies (anti-TPO, TRAb, anti-Tg) were negative. The biochemical trend and clinical context made destructive thyroiditis and iodine-induced hyperthyroidism unlikely. Screening for catecholamine excess, porphyria, metabolic and rheumatologic disorders was negative. Further diagnostic assessments are ongoing to investigate a possible underlying endocrinological syndrome. During hospitalization, the patient experienced recurrent chest/epigastric pain with limited response to analgesics; serial ECGs showed dynamic ST-segment elevation with recurrent troponin rises. Cardiac magnetic resonance demonstrated mildly reduced ejection fraction (44%), diffuse myocardial edema and subepicardial late gadolinium enhancement with a ring-like apical pattern, consistent with acute myocarditis. Guideline-directed therapy for ventricular dysfunction and thyrostatic treatment were initiated, with initial improvement. The patient was discharged with indication for strict follow-up; however, subsequent clinical evolution could not be assessed due to loss to follow-up. Conclusion. This case supports the relevance of a structured diagnostic approach in STEMI-like presentations with non-obstructive coronary arteries and suggests a possible association between thyrotoxicosis and acute myocarditis.