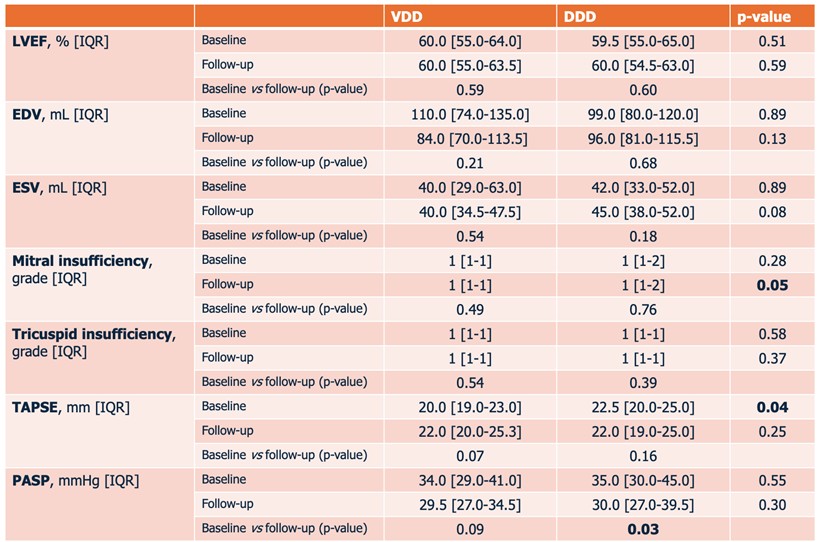
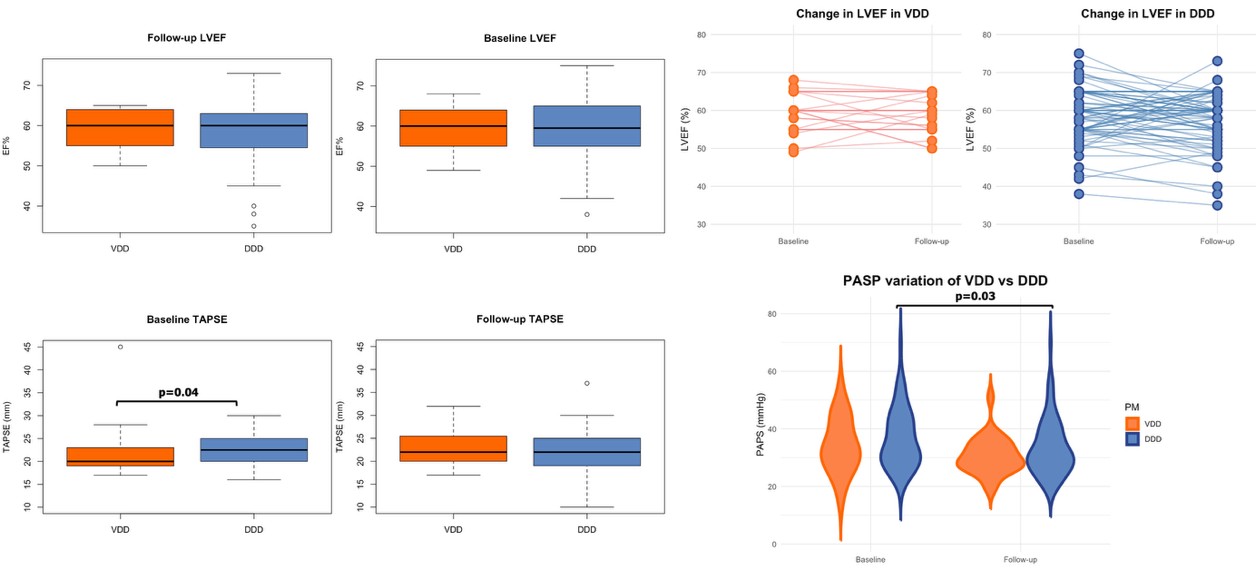
Background. In patients undergoing transcatheter aortic valve replacement (TAVR), subsequent pacemaker (PM) implantation has been associated with worsening ventricular function and higher heart failure hospitalization rates. Evidence remains scarce about the long-term effects of single lead atrioventricular sequential (VDD) pacing on left and right ventricular function as compared to dual lead (DDD) pacing. Purpose. We hypothesized that, in patients undergoing PM implantation following TAVR complications, VDD are not significantly different from DDD concerning left and right ventricular function variation over time, as well as native valvular regurgitation. Methods. Patients who underwent VDD or DDD implantation secondary to TAVR complications were retrospectively enrolled. Baseline demographic and echocardiographic data were collected the day before TAVR. Clinical reassessment with echocardiography was performed every six months; for each subject. Results. One hundred eleven patients were enrolled (27 [24%] VDD and 84 [76%] DDD). The population was mainly composed by men (17 [63%] VDD vs. 44 [52%] DDD, p=0.46), presenting with baseline electrocardiographic alterations (17 [63%] VDD vs. 52 [62%] DDD, p=0.93), with a median New York Heart Association (NYHA) class of II (interquartile range, II-III; p=0.49) and a preserved left ventricular ejection fraction (LVEF, 60.0% [55.0-64.0] in VDD vs. 59.5% [55.0-65.0] in DDD, p=0.51). Notably, VDD patients were older than DDD patients (85.0 [81.5-88.0] vs. DDD 82.0 [78.8-85.0] years, p=0.01). Median follow-up time was 1120.0 [823.0-1302.0] days (VDD 1034.5 [895.3-1428.5] vs. DDD 1123.5 [796.3-1277.0] days; p=0.87). Baseline and follow-up echocardiographic data are detailed in Figure 1 and graphically summarized in Figure 2 . Median NYHA class at follow-up was similar between groups (class I [I-II] for both groups, p=0.88), and significantly lower than baseline (p<0.001). Notably, echocardiography parameters were substantially stable over time (LVEF 60.0% [55.0-63.5] in VDD, p=0.59; 60.0% [54.5-63.0] in DDD, p=0.60), except for a significant decrease of pulmonary arterial systolic pressure (PASP) from baseline in DDD (35.0 [30.0-45.0] vs. 30.0 [27.0-39.5] mmHg, p=0.03). Conclusions. This retrospective analysis of TAVR patients suggests that VDD pacing provides comparable echocardiographic outcomes to DDD pacing, with both groups maintaining stable left and right ventricular function over long-term follow-up.