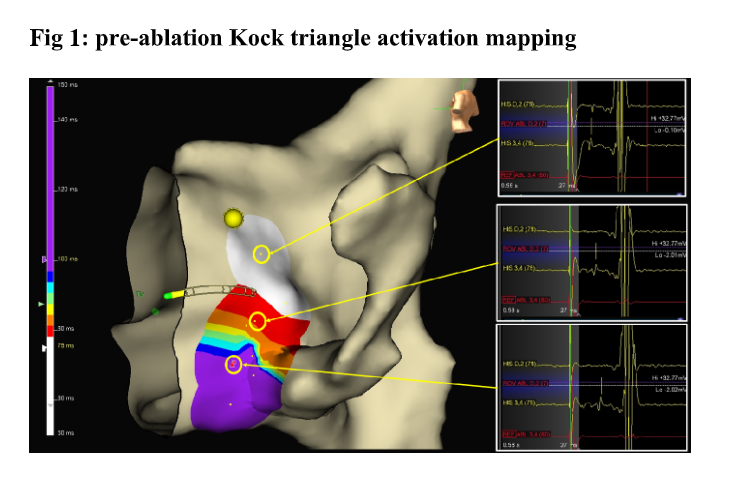
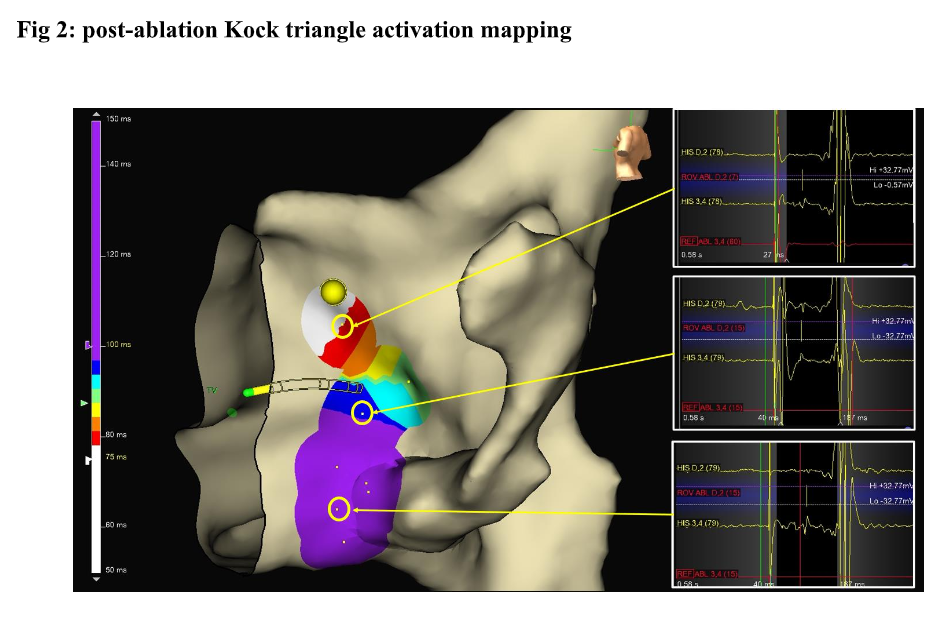
Introduction Slow pathway ablation is currently the target for AV nodal reentrant tachycardia (AVNRT) with a high success rate. Kock triangle (KT) mapping is helpful to define the fast pathway location. We aimed to describe the KT mapping by means of electroanatomic (EA) local activation mapping (LAT) technique of fast pathway location performed beside the conventional EP mapping. Methods KT was mapped as follows: atrial pacing from peri-Hisian antero-septal (AS), mid-septal (MS) and postero-septal (PS) regions, by means of 4 mm ablating catheter beside a quadripolar diagnostic catheter placed on His region. The LAT was performed by means of Ensite X system (Abbott Medical) in all patients; the window of interest was set from 10 msec after the pacing atrial spike to the ventricular EGM on the His catheter tracing. The spike-to-His deflection (S-H) interval was measured to define the fast pathway location and activation gradient. On the ablator catheter tracing the annotation was set (ROV), timed to the His deflection on His tracing. The annotation was set even when no His deflection was recorded on ablator tracing as in MS and PS regions (“mirroring”). The KT was mapped before and after successful elimination of the slow pathway Results Seventeen consecutive AVNRT patients were included who underwent to a successful slow pathway elimination. In all cases, at baseline pre-ablation mapping a progressive prolonged S-H interval was found (AS<MS<PS) depicted as activation gradient, traditionally meaning as anteroseptal fast pathway physiologic location, confirmed by the EA LAT (Fig 1). As compared to pre-ablation, the post-ablation LAT mapping showed the same activation gradient in all patients (Fig 2). Conclusion KT mapping by means of LAT, may help to define the AV node dual physiology beside the conventional EP mapping; it may also define a safer region for slow pathway ablation.