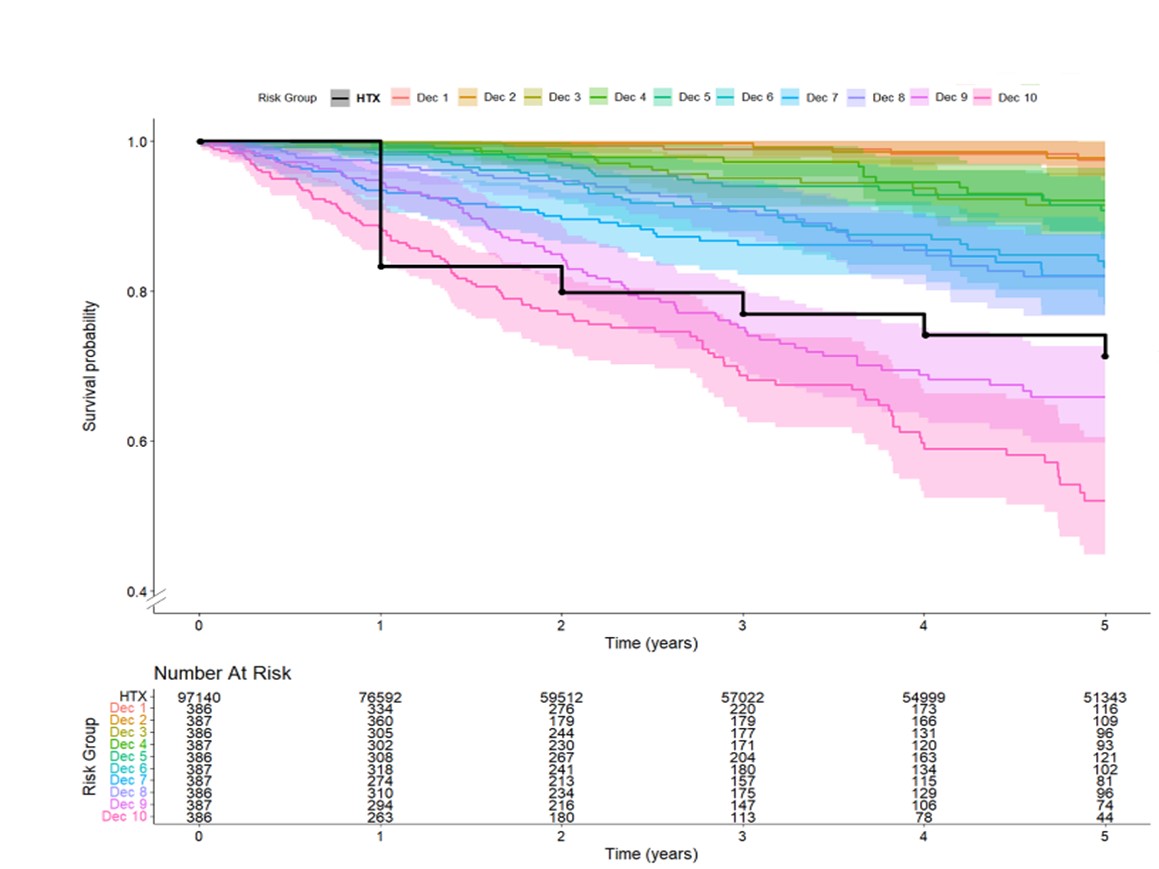
Background. In patients with chronic heart failure (HF), current guidelines recommend the use of prognostic scores to estimate survival and to support referral for heart transplantation (HTX). However, the clinical use of these tools remains limited, and no universally accepted cut-off values are currently available to guide transplant listing. Among the available scores, the MECKI score – based on easily obtainable parameters (peak VO₂, VE/VCO₂ slope, hemoglobin, sodium, left ventricular ejection fraction, and glomerular filtration rate) – has shown one of the highest prognostic accuracies. Aim. The aim of this study was to compare the survival of patients enrolled in the MECKI score registry with that of heart transplant recipients reported in the ISHLT registry, and to identify a MECKI score threshold beyond which 5-year prognosis is worse than that of HTX recipients. Methods. Consecutive ambulatory HF patients included in the MECKI score program between January 2010 and January 2022 were analyzed. The primary endpoint was a composite of cardiovascular death, HTX, or left ventricular assist device implantation. Post-HTX survival data were obtained from the International Society of Heart and Lung Transplantation (ISHLT) registry updated through 2023. To identify the prognostic threshold, patients were stratified by MECKI score deciles. Results. A total of 3,865 patients were evaluated (mean age 62.4±12.6 years). Mean peak VO₂ was 58.2±18.3% predicted; mean VE/VCO₂ slope 33.2±8.2; hemoglobin 13.5±1.7 g/dL; sodium 139±3 mmol/L; LVEF 33.7±10.4%; eGFR 73±26 mL/min/1.73 m². Periodic breathing was observed in 15.8% of cases. At 5 years, overall survival was 83.7%. The mean 5-year survival of HTX recipients (71.2%) fell between the 8th and 9th MECKI score deciles, identifying a threshold value of 0.1368 as the point beyond which prognosis becomes worse than that of transplant recipients. Conclusion. A MECKI score ≥0.1368 may represent a reliable threshold for referral to HTX evaluation, whereas lower values are associated with survival comparable to or better than transplantation, thus supporting deferral of listing. Incorporating the MECKI score into routine clinical practice could enable a more rational and timely selection of transplant candidates, addressing a current gap in guideline recommendations.