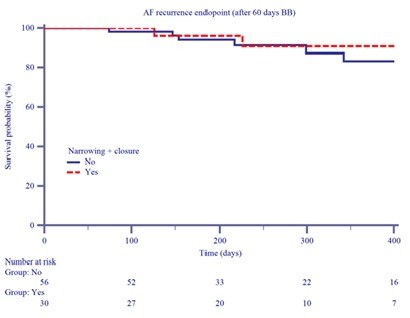
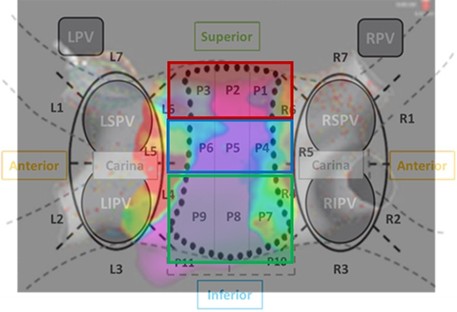
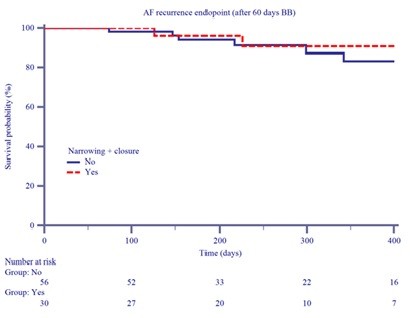
Pulsed-field ablation (PFA) is a non-thermal ablation technology potentially more selective and safer than traditional techniques; however, the extent of lesion formation and the unintentional involvement of the left atrial (LA) posterior wall (PW) remain unclear. This study aimed to characterize PFA lesion formation after pulmonary vein isolation (PVI) in real-world atrial fibrillation (AF) patients using high-density (HD) voltage mapping, and to evaluate whether unintentional PW involvement is associated with arrhythmia recurrence. A total of 113 patients were prospectively enrolled and underwent PVI using the Farapulse PFA system at 14 centers. Protocol-directed PVI was delivered at 2 kV with eight applications per vein, with additional applications at the operator’s discretion. After PVI, an HD three-dimensional LA map was acquired using Rhythmia/Orion (31%), Carto/Pentaray (29.2%) or NavX/HD Grid (39.8%) systems. Bipolar voltage maps were displayed using a <0.5 mV threshold to identify low-voltage areas zones as either acute lesion formation or chronic scarring. Pulmonary veins were segmented into seven sectors for regional analysis. To quantify PW lesion extension, nine predefined PW sectors were grouped into upper, intermediate and lower segments. Unintentional PW involvement was defined as involvement of at least one PW sector; PW narrowing as involvement of two sectors within the same segment, and PW closure as involvement of all three sectors within a segment. Patients were followed for a median of 280 days. PVI was successfully achieved in all patients, with complete antral isolation in 100% of cases. The mean ablated area around PVs was 34.3±5 cm 2 : 10.0±4 cm 2 at the anterior portion of the PVs, 9.2±2 cm 2 at the posterior site, 4.2±1 cm 2 in the superior area, 3.9±1 cm 2 in the inferior area and 5.3±2 cm 2 at the carina region. Unintentional PW involvement occurred in 63 patients (55.8%), including PW narrowing in 31 (27%) and PW closure in 8 (7%). During follow-up, 10.4% experienced AF recurrence and 8.1% developed atrial tachycardia or flutter. No significant association was found between PW involvement and arrhythmia recurrence. PW involvement after PFA-based PVI is frequent but does not appear to increase arrhythmia recurrence risk. Larger prospective studies with longer follow-up are needed to clarify its clinical relevance.