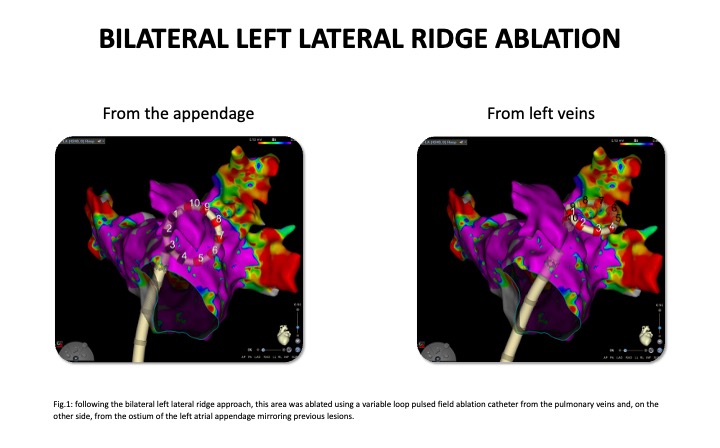
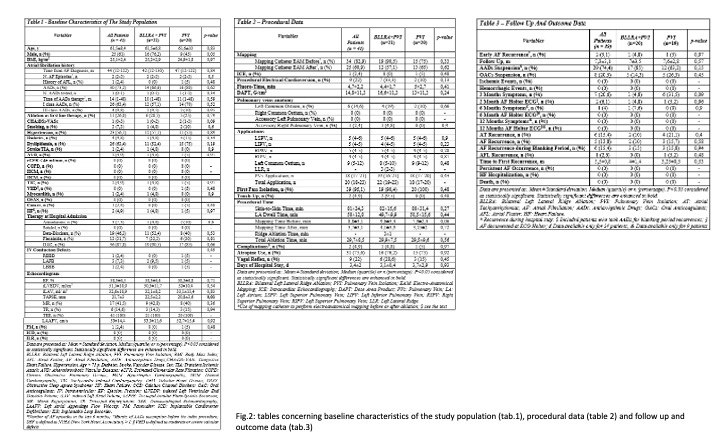
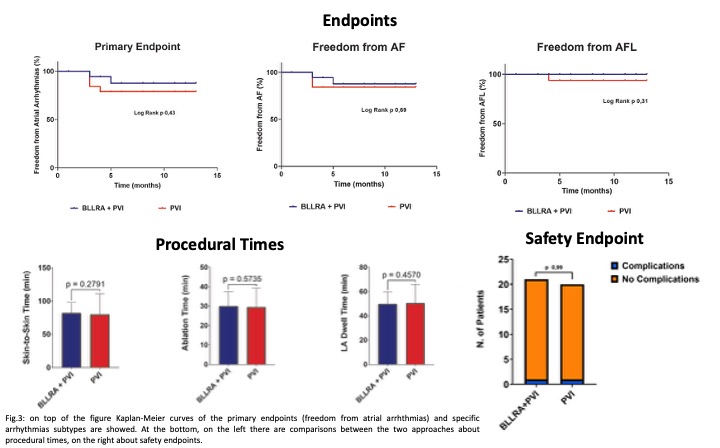
Background Left lateral atrial ridge (LLR) is a crossroads of different tissues, known as a substrate for atrial fibrillation (AF) triggers, but also as a challenging ablation site. We previously proposed the bilateral ablation approach. Purpose The aim of this study is to assess the feasibility, safety and efficacy of adding bilateral ablation of the left lateral ridge (BLLRA) to pulmonary vein isolation (PVI) in preventing AF recurrences. Methods We designed a 1:1 randomized, single-blinded, superiority trial enrolling consecutive patients undergoing first paroxysmal AF ablation. Patients were randomized to BLLRA plus PVI (fig.1) or to PVI only, performed using a variable loop pulsed field ablation catheter. The primary endpoint is freedom from atrial tachyarrhythmias 12 months after ablation. The secondary endpoint is a safety outcome. The sample size was calculated 121 patients per group. A structured follow up at 2, 6 and 12 months was settled. This is an interim analysis of the preliminary results. Results In this preliminary analysis, a total of 41 patients (mean age 61,5±8,4; male 61%) were enrolled from October 2024 to September 2025. 21 patients (mean age 61,5±6,8; male 76,2%) were randomized in BLLRA plus PVI group, whilst 20 patients in the PVI group (mean age 61,5±10; male 45%). Baseline characteristics were balanced between groups (fig.2). Two patients did not start the follow up. No differences were documented between groups about procedural data nor times (fig.2 and 3). After 7,3±3,1 months of follow up, freedom from recurrent atrial arrhythmia (fig.3), without the use of antiarrhythmic drugs and after 8 weeks of blanking period, was present in 18 of 20 patients (90%) assigned to BLLRA plus PVI, compared with 15 of 19 (78,9%) assigned to PVI alone (between-group difference, –11,9%; hazard ratio [HR], 0.52 [95% CI, 0.10-2,59]; log rank p = 0,43). Evaluating the type of arrhythmia, freedom from AF was documented in 90% of patients of the intervention group and 84,3% of the control group (log rank p = 0,69); whereas freedom from atrial flutter occurred in 100% of BLLRA plus PVI group and 94,8% in PVI only group (log rank p = 0,31). No events of the safety outcome occurred, except for two vascular minor complications. Conclusions BLLRA plus PVI is a feasible and safe treatment for paroxysmal AF. There is a favorable trend toward efficacy when compared to PVI only, but more data, patients and time are needed.