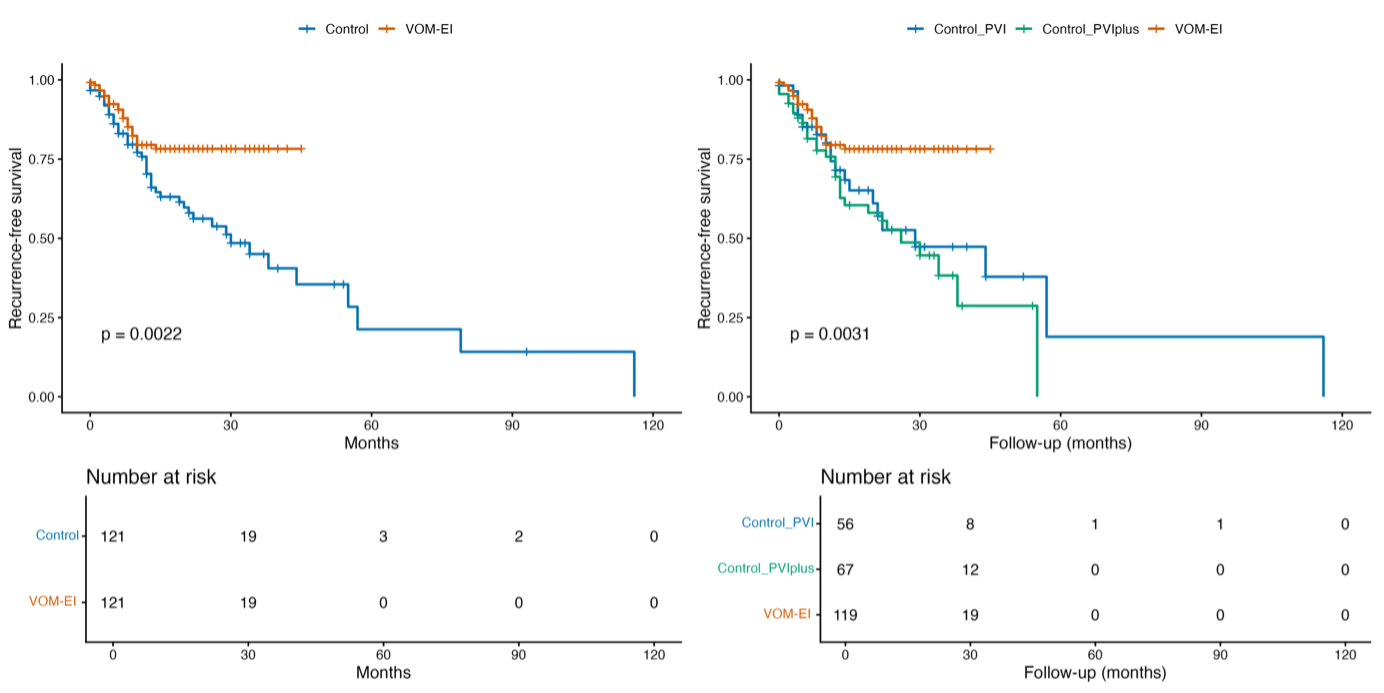
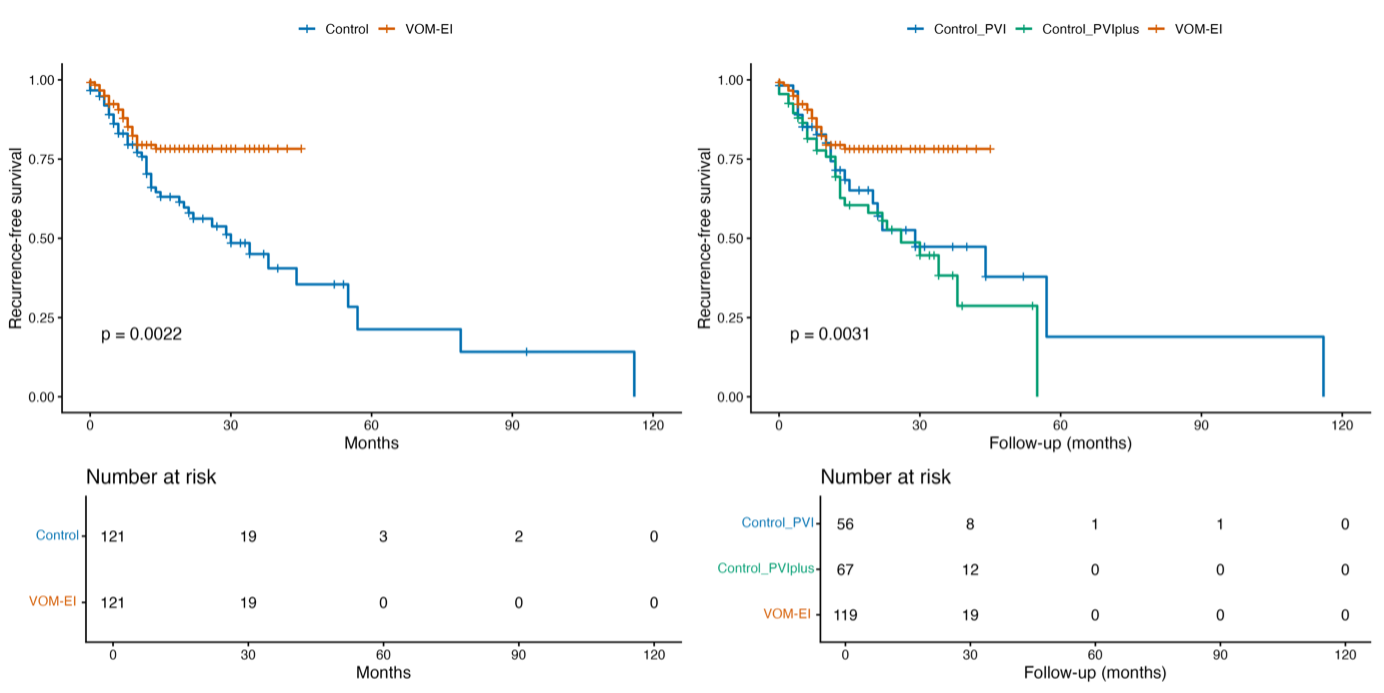
Background The optimal ablation strategy for patients undergoing repeat catheter ablation (CA) for atrial fibrillation (AF) remains debated. Vein of Marshall ethanol infusion (VOM-EI) has been proposed to enhance substrate modification and improve long-term rhythm control, particularly in persistent AF, but its role in repeated ablations is poorly investigated. Purpose To evaluate whether adding VOM-EI to a standardized ablation setup during repeat AF ablation improves long-term rhythm outcomes compared with standard redo strategies. Methods In this retrospective, multicenter observational study, consecutive patients undergoing repeat CA for AF were included. The VOM-EI approach consisted of ethanol infusion followed by systematic completion of a predefined ablation setup (verification of PV isolation and assessment of conduction block across lateral mitral isthmus, left atrial dome and cavotricuspid isthmus). Patients were first analyzed as VOM-EI vs non-VOM redo procedures. Propensity score matching was conducted using demographic and arrhythmia-related covariates. The primary endpoint was recurrence of atrial tachyarrhythmias >30 seconds. Time-to-event outcomes were evaluated with Kaplan–Meier analysis and Cox regression. Secondary analysis stratified patients into three strategies—PVI-only, PVI plus substrate modification, and VOM-EI setup—comparing outcomes using inverse probability of treatment weighting (IPTW). Results A total of 263 patients undergoing repeat ablation were included (28% long-lasting persistent AF). Of these, 121 underwent VOM-EI and 142 standard redo strategies (60 PVI-only, 82 PVI plus substrate modification). After matching, 111 VOM-EI patients were compared with 111 controls. Atrial arrhythmia recurrence occurred in 42% of controls vs 20% of VOM-EI patients. In multivariate Cox regression, the VOM-EI+anatomical strategy was associated with a significantly lower risk of recurrence (HR 0.32, p=0.0001), independent of age, AF duration, and previous procedures. In IPTW analysis, VOM-EI+anatomical strategy showed favorable outcomes compared with both PVI-only and PVI plus substrate modification, with greatest benefit in patients with long-lasting AF. Conclusions This observational multicenter study using matched cohorts shows that VOM-EI combined with a specific predefined anatomical ablation setup is associated with improved long-term outcomes compared with standard redo strategies in a large persistent AF population.