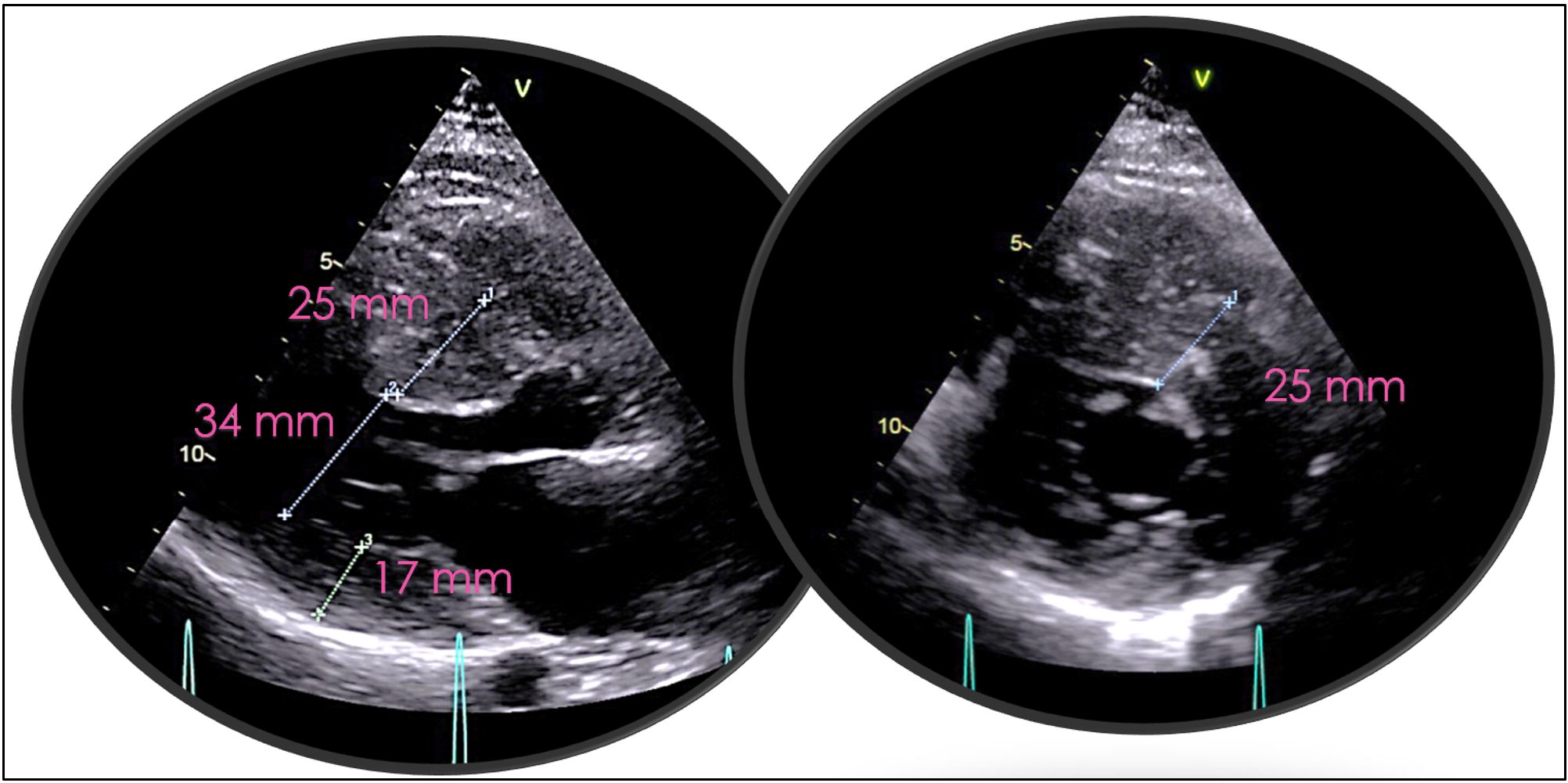
Introduction Hypertrophic cardiomyopathy (HCM) is a genetically heterogeneous myocardial disease characterized by marked phenotypic variability, even among carriers of the same pathogenic mutation. Pregnancy in women with obstructive HCM represents a high-risk condition, particularly in the presence of severe left ventricular outflow tract (LVOT) obstruction and limited pharmacological options. We report a case highlighting the challenges of risk stratification and management of obstructive HCM during pregnancy. Case Presentation A 24-year-old woman with a family history of HCM was referred for cardiological evaluation during the third month of pregnancy. Genetic testing identified a pathogenic MYH7 variant (c.1987C>T, exon 18), shared with her mother and sister. Marked intrafamilial phenotypic variability was observed, with both obstructive and non-obstructive HCM phenotypes; the patient’s mother and grandmother were obstructive, whereas her sister was non-obstructive, and the patient showed cardiac involvement from the neonatal period. At presentation, she reported dyspnea on mild-to-moderate exertion (NYHA class III). Electrocardiography showed left atrial enlargement and left ventricular hypertrophy with secondary right ventricular repolarization abnormalities (Fig. 1). Transthoracic echocardiography revealed severe concentric hypertrophy (septal thickness 25 mm), grade II diastolic dysfunction, systolic anterior motion of the mitral valve, and severe LVOT obstruction with a peak gradient >150 mmHg (Fig. 2). Due to the high maternal risk and limited pharmacological options during pregnancy, close outpatient monitoring was adopted. Given an estimated HCM sudden cardiac death risk of 6.62%, a subcutaneous implantable cardioverter-defibrillator was implanted during pregnancy. The patient completed pregnancy without major complications and delivered at term by elective cesarean section. Postpartum optimization of medical therapy led to symptomatic improvement (NYHA II). Subsequently, CYP2C19 genotyping was performed to evaluate potential eligibility for treatment with the cardiac myosin inhibitor mavacamten. Conclusion This case underscores the complexity of managing obstructive HCM during pregnancy, emphasizing the importance of early risk assessment, multidisciplinary care, and individualized management strategies, particularly in patients with severe LVOT obstruction and significant intrafamilial phenotypic variability.