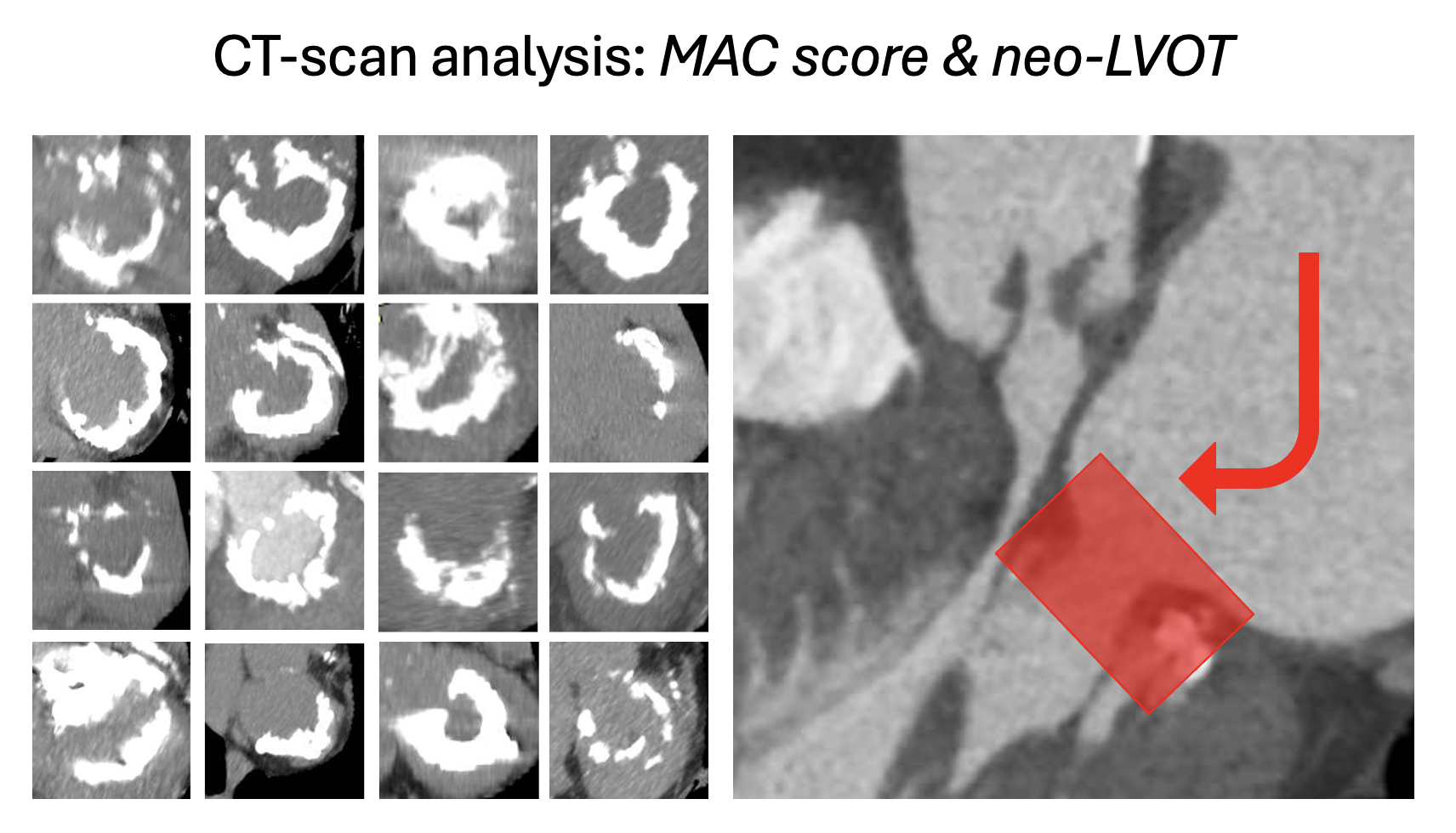
Background A clear standard for the treatment of mitral annular calcification (MAC) has yet to be established. Conventional surgical strategies continue to be associated with high mortality rates, whereas percutaneous Valve-in-MAC (ViM) procedures have shown promising results, although still limited by the risks of LVOT obstruction, embolization, and apical perforation. In recent years, several reports have described hybrid surgical “off-label” implantation of an aortic transcatheter heart valve (THV), proposed ad a way to mitigate these risks through more controlled device deployment. Here, we present our single-center experience of transatrial direct surgical Valve-in-MAC (TADS-ViM). Methods Between July 2022 and October 2024, n=16 patients affected by severe mitral valve steno-regurgitation underwent TADS-ViM. A mini-thoractotomy access was performed in one subject. On CPB, the anterior leaflet was removed and single- or bi-commissural sutures were applied in all cases to reduce valve area and circularize the annulus. After pre-dilatation, a SAPIEN 3 Ultra THV was inflated ~30/70% atrio-ventricular, commissurally aligned. Four-to-nine single atrial U-stitches were placed to avoid embolization. An eventual post-dilatation was performed to improve stent frame expansion after knot tying. Results Procedural success rate was 100%. CT-scan analyses confirmed severe MAC (score: 8.5 [7,9]; area: 607±97 mm2, predicted neo-LVOT: 205 [165, 283] mm2, n=2 complete obstruction). Median clamp time was 89 [68, 125] min. A 26 and 29 mm devices were implanted in n=5 and n=11 patients, respectively. 50% of the patients underwent concomitant procedures (n=6 AVR; n=4 CABG; n=2 aortic surgery). No cases of LVOT obstruction were reported, but one patient required revision for major bleeding due to apex lesion during balloon inflation. 30-day mortality rate was 18.8% (n=3), mainly due to sepsis. At a median follow-up of 1 year, survival rate was 75% (n=12). One patient required percutaneous closure of bi-commissural leaks at 2.5 years. Conclusions TADS-ViM may represent a valid alternative to complex surgical decalcification strategies or challenging ViMAC procedures. Concomitant targets may also be surgically addressed and small anatomies -not amenable of percutaneous approach- treated as well. However, mortality rate of these fragile and comorbid patients remains high. The implementation of less invasive and durable solutions to treat MAC is mandatory.