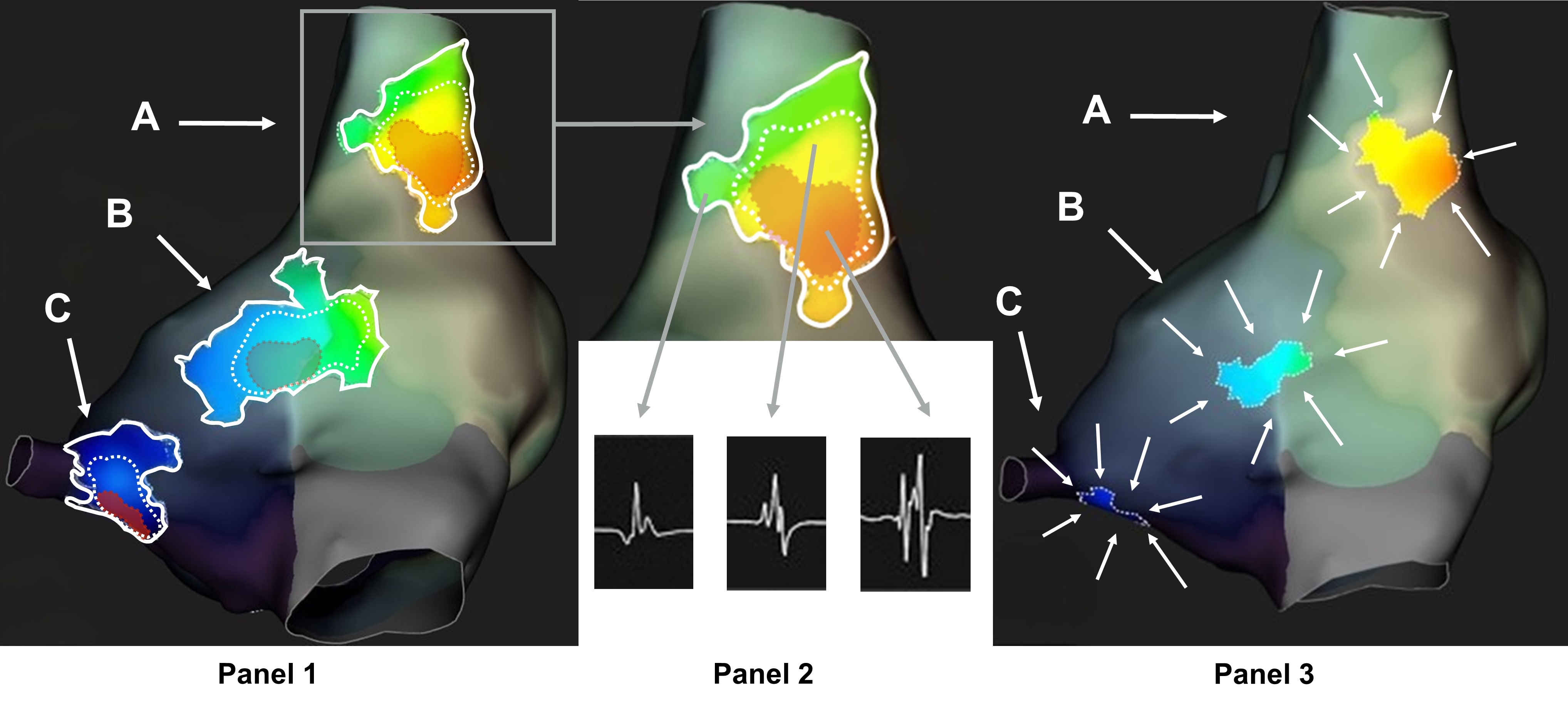
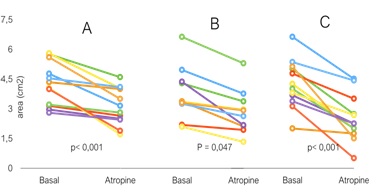
Background and aims: Ganglionated plexi (GPs) are the primary target of ablative therapies for neurally mediated syncope (NMS); however, the optimal method for their endocardial localization remains unclear. This study analyzed bipolar atrial electrograms (EGMs) and their response to a vagolytic agent to elucidate their relationship with the parasympathetic network. Methods: High-density right atrial mapping was performed before and after 2 mg atropine in healthy patients without structural heart disease undergoing electrophysiological study for standard indications. Offline analysis compared pre- and post-atropine maps, focusing on fragmentation patterns and spectral analysis. Results: The study included 13 patients (mean age: 34±12 years, 9 males). Baseline maps exhibited a consistent fragmentation pattern in the posterior-septal wall, reflecting anatomical right GPs distribution. No difference in density of points between the pre-post atropine map was detected (p=0.97). Three primary areas were identified in the supero-(A) , mid-(B) , and infero-posterior-(C) regions. Fragmentation of EGMs was found to increase from the periphery toward the core of each area. In fact, the fragmentation pattern was consistent across all analyzed GPs areas: a centrally located, rounded high-fragmentation area (≥6 deflections) was surrounded by a low-fragmentation area (≥4 deflections), with a transition zone (≥5 deflections) in between ( Figure 1 ). Atropine significantly reduced fractionated areas (p<0.001 for A and C, p<0.05 for B, Figure 1, Figure 2 ). External areas exhibited "functional" fragmentation, sensitive to vagal output, whereas central cores displayed "structural" fragmentation, resistant to vagolysis. Conclusion: Fragmentation of atrial EGMs is a dynamic property, related to parasympathetic output. Standard fragmentation criteria may overestimate GPs areas. These results could suggest a more selective approach on central core of GPs during Cardioneuroablation procedure, potentially reducing procedural risks and improving long-term outcomes.